Advertisement
Advertisement
May 2021 Supplement
Sponsored by Philips
Case Report: Treatment of Severe Calcific CLI With Atherectomy, Scoring Balloon Angioplasty, and the Tack Endovascular System
CASE PRESENTATION
A woman in her mid 60s with prior history of end-stage renal disease on dialysis, diabetes mellitus on insulin, hypertension, and prior left transmetatarsal amputation presented with extensive Rutherford class 5 right digital gangrene. On physical examination, the patient had nonpalpable pedal pulses with monophasic dorsalis pedis (DP) artery Doppler signals. Noninvasive studies demonstrated a minimally pulsatile ankle pulse volume recording with flat transmetatarsal and digital waveforms.
PROCEDURAL OVERVIEW
The patient was taken to the operating room for angiography and possible intervention. Contralateral groin access was achieved. Initial angiography demonstrated popliteal artery occlusion of the P2 segment with an eccentric calcific lesion (Figure 1A). Distally, the patient had long-segment stenosis with multifocal occlusion of the proximal anterior tibial artery and occluded peroneal and posterior tibial arteries (Figure 1B). In the foot, the primary outflow was a diminutive DP artery. After heparinization and sheath access, initial attempts were made to cross the lesion antegrade. Using a 0.018-inch Quick-Cross catheter (Philips) and a 0.014-inch hydrophilic tip wire, we successfully navigated past the popliteal occlusion and into the distal popliteal artery. The proximal anterior tibial artery was accessed, but we were unable to cross the long-segment lesion in the proximal anterior tibial artery via an antegrade approach. Pedal access of the DP artery was then obtained, and the lesion was successfully crossed retrograde with a 0.014-inch guidewire and a 0.018-inch Quick-Cross catheter. Through and through wire access was obtained.
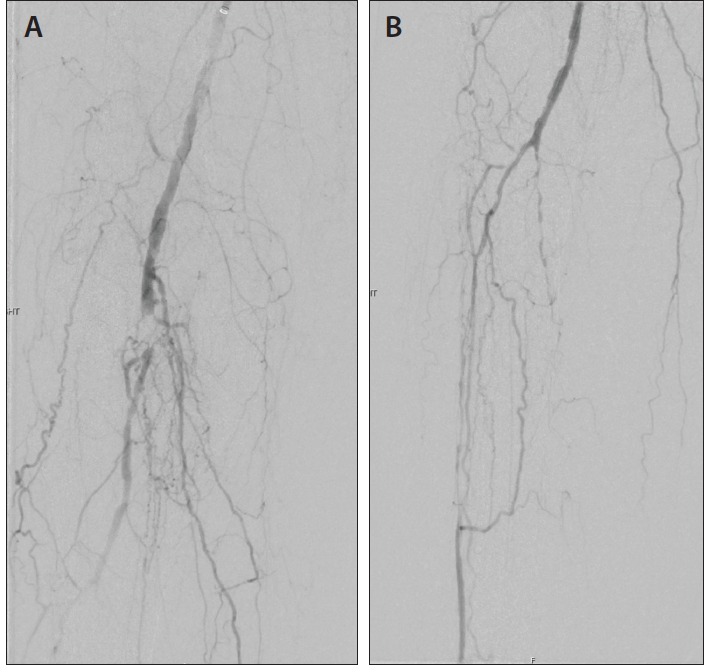
Figure 1. Pretreatment images show the eccentric popliteal occlusion (A) as well as the extensive proximal tibial disease (B).
Focal atherectomy of the eccentric calcific occlusion at the P2 popliteal artery was then performed with a 2.2-mm Phoenix atherectomy device (Philips). Two passes were completed without difficulty, with noted improvement in luminal gain and distal filling. AngioSculpt PTA Scoring balloon catheter (Philips) was then inflated to 5 mm, followed by drug-coated balloon angioplasty with prolonged inflation. Significant improvement was noted in the luminal diameter and flow, with minimal residual plaque and no evidence of dissection (Figure 2).
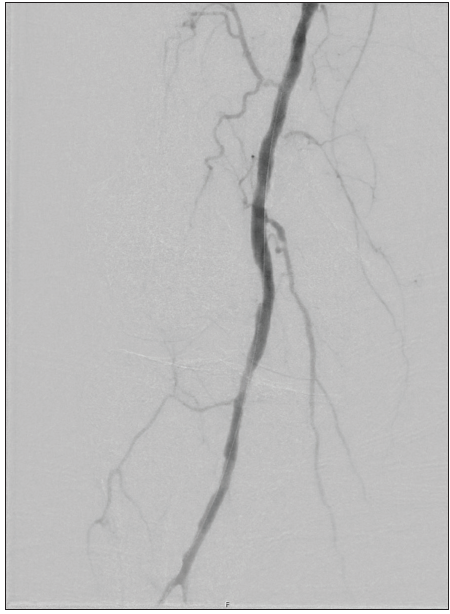
Figure 2. Significant improvement in luminal diameter and flow in popliteal artery following Phoenix atherectomy and use of Angiosculpt scoring balloon.
Attention was then turned to the anterior tibial artery lesion. Plain balloon angioplasty with sustained inflation was performed to 2.5 mm. Subsequent angiography demonstrated a widely patent anterior tibial artery. There were two areas of focal grade B dissection (Figure 3A). We suspected these may represent entry/reentry points from our retrograde access. Given the limited patency of primary balloon angioplasty below the knee, we elected to place two 4-F, 6-mm Tack implants (Philips) at the areas of dissection (Figure 3B). Completion angiography demonstrated brisk filling of the DP in the foot (Figure 3C). Follow-up noninvasive studies demonstrated substantial improvement in pulsatility with a widely patent popliteal and anterior tibial arteries. The patient successfully underwent podiatric transmetatarsal amputation with complete healing at most recent follow-up.
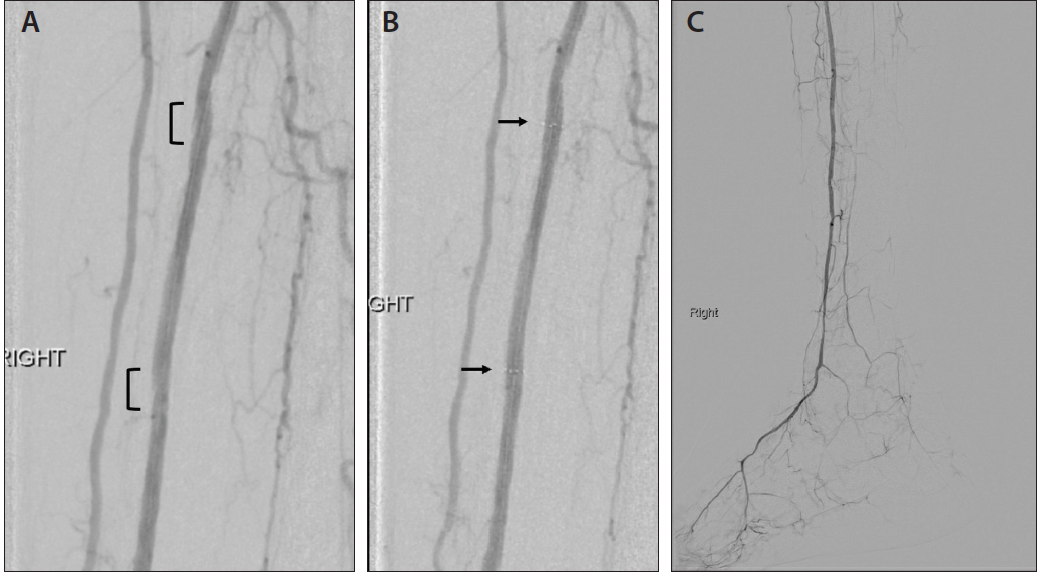
Figure 3. Post-tibial angioplasty showed two grade B dissections (A) successfully treated with two 4-F Tack implants (B). Completion angiogram of the popliteal artery and foot show in-line flow to the DP (C).
DISCUSSION
Current management strategies for severe calcific disease of the infrageniculate arteries are limited by durability and patient fitness. In this case, we felt this patient was not a candidate for open bypass given her comorbid conditions. To decrease the need for bailout stenting of the popliteal artery, luminal gain with the front-cutting Phoenix atherectomy device and AngioSculpt scoring balloon resulted in excellent vessel preparation for subsequent drug-coated balloon angioplasty. In the tibial vessels, use of the 4-F Tack device allowed us to improve the long-term patency of traditional below-the-knee plain balloon angioplasty by targeting focal dissections.
Advertisement
Advertisement
